Clinical Scenario:
Patient is a 19-year-old female, collegiate ice hockey goaltender who sustained a concussion during a game ~3 weeks prior when she was run into by an opposing player and subsequently hit her head on the ice. Her chief complaint at time of evaluation was persistent symptoms of dizziness, headache and neck pain, all of which had prevented her from performing daily academic and personal responsibilities. Patient denied loss of consciousness at the time of injury and reports imaging revealed no fractures.
Key Exam Findings:
DHI: 36/100
NPRS: headache 2/10, dizziness 3/10, neck pain 3/10; pt reports all increase with activity
PCSS: 36
Oculomotor Exam: Pupils are reactive and symmetrical, with full visual fields. Pt demo normal smooth pursuit however was unable to perform >5 rapid alternating eye movements before exacerbation of symptoms. Pt demo 3-line difference during Dynamic Visual Acuity test, with c/o dizziness with head movement horizontally > vertically.
Gait and Balance: Pt demo increased sway with tandem stance as well as increased sway and reduced time bilaterally during single leg balance on firm surface with eyes closed. Romberg test negative. Pt demo normal gait pattern however was unsteady during tandem gait backwards > forwards. Tandem gait worse with eyes closed.
Palpation: TTP at C/S paraspinals
Other: Head thrust, Dix-Hallpike and Roll tests all negative. No dysmetria observed in upper or lower extremities. Strength and sensation WNL throughout.
PICO Question:
In adolescent and young adults (ages 13-25) with reports of dizziness and headache following a sport-related concussion, does cervical and vestibular rehabilitation have a greater impact on symptom reduction than rest alone?
Search Strategy:
A literature search was performed to identify all eligible articles, including randomized controlled trials, cohort studies, and case studies. Electronic searches of MEDLINE (January 2002-August 2016), Pedro, and CINAHL (2006-2016) were performed, using keywords ‘concussion’, ‘brain concussion’, ‘physical therapy’, ‘vestibular’, ‘rest’, ‘physical therapy modalities’, and ‘sport-related concussion’. Only full reports in English, peer reviewed, and human trials were included. Initial search strategy was to included on randomized controlled trials investigating concussions with physical therapy treatment aimed at comparing cervicovestibular treatment to rest or standard treatment protocols in the adolescent and young adult population; however, due to lack of current/emerging research for this topic, the level of study as well as age range was expanded to include adolescent and adult populations. Articles were excluded if they did not specify or include reference to physical therapy treatment following concussion or mild traumatic brain injury for acute and/or persistent post-concussion symptoms including headache, dizziness, and/or neck pain.
58 Articles Identified through Search => 44 Articles excluded after screening titles/abstracts => 14 Full Texts Reviewed => 9 Articles excluded (lack of treatment or relevant outcome measures, lower quality evidence) => 5 Articles Included
Results:
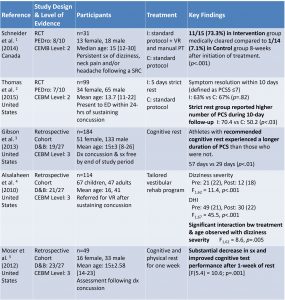
Clinical Bottom Line:
The current evidence available to address treatment for persistent symptoms of dizziness and headache following a sport-related concussion is minimal. In the studies reviewed to address the clinical question, there was inconclusive evidence to support the theory that cervical and vestibular rehabilitation are more beneficial than rest alone in reducing symptoms following a sport-related concussion. There were two studies available that addressed cervical and vestibular therapy as treatment for post-concussion symptoms (1 RCT and 1 retrospective analysis), and although there were positive findings as to the effectiveness of this type of treatment, limitations in sample size, treatment protocols and lack of analysis on the effects of covariates such as age, time, and dosage of treatment, impact the overall quality of the findings. Low-quality evidence does suggest that for symptoms persisting longer than 10 days, strict cognitive and physical rest may not be as beneficial in symptom reduction as beginning a low-level, multi-modal physical therapy treatment plan. However, these studies were retrospective in nature and lacked randomization and control or comparison groups. For patients with persistent post-concussion symptoms presenting with cervical and/or vestibular dysfunction, an early rest period followed by an impairment-based treatment program with gradual progression may help facilitate recovery.
Application to Case Scenario:
- Patient is outside spontaneous recovery window (~7-10 days post-injury); study by Gibson et al. suggests additional cognitive rest not indicated
- Studies by Schneider et al. and Alsalaheen et al. suggest individualized VR program may be beneficial in symptom reduction
- Plan of care: 2x/week for 6-8 weeks
- Intensity: Symptom exacerbation ≤ 15-30 min
- Interventions: aerobic training, balance, adaptation and substitution exercises, C/S AROM and manual therapy
Limitations:
- Lack of available high-quality evidence
- 3 of 5 articles were retrospective studies and lacked control groups
- Lack of long-term follow-up and formal vestibular function testing
- Future Research: High-quality RCT’s with focus on short- and long-term effects of VR on PCS
References:
- Schneider K, Meeuwisse W, Emery C, et al. Cervicovestibular rehabilitation in sport-related concussion: a randomised controlled trial. British Journal Of Sports Medicine [serial online]. September 2014;48(17):1294-1298.
- Thomas D, Apps J, Hoffmann R, McCrea M, Hammeke T. Benefits of Strict Rest After Acute Concussion: A Randomized Controlled Trial. Pediatrics [serial online]. February 2015;135(2):213-223. Available from: CINAHL, Ipswich, MA.
- Gibson S, Nigrovic L, O’Brien M, Meehan W. The effect of recommending cognitive rest on recovery from sport-related concussion. Brain Injury [serial online]. July 2013;27(7/8):839-842. Available from: CINAHL, Ipswich, MA.
- Alsalaheen B, Mucha A, Sparto P, et al. Vestibular rehabilitation for dizziness and balance disorder after concussion. Journal Of Neurologic Physical Therapy [serial online]. June 2010;34(2):87-93. Available from: CINAHL, Ipswich, MA.
- Moser R, Glatts C, Schatz P. Efficacy of immediate and delayed cognitive and physical rest for treatment of sports-related concussion. Journal Of Pediatrics [serial online]. November 2012;161(5):922-926. Available from: CINAHL, Ipswich, MA.
- Daneshvar D, Nowinski C, McKee A, Cantu R. The epidemiology of sport-related concussion. Clinics In Sports Medicine [serial online]. January 2011;30(1):1-17. Available from: CINAHL, Ipswich, MA.
- Ellis M, Cordingley D, Vis S, Reimer K, Leiter J, Russell K. Vestibulo-ocular dysfunction in pediatric sports-related concussion. JOURNAL OF NEUROSURGERY-PEDIATRICS. 2015;16(3):248-255. doi: 10.3171/2015.1.PEDS14524.