Background Information:
- 4% of spinal cord injuries (SCI) lead to chronic mechanical ventilation
- Mechanical ventilation, currently the gold standard for respiratory dependent patients, has many potential complications
- Serious complications include:
- Pneumonia, the leading cause of decreased life expectancy amongst this population
- Respiratory Infection
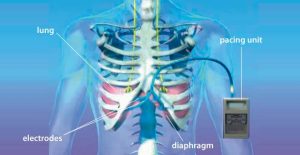
- Via transcutaneous electrical stimulation, the patency of the phrenic nerve can be determined preoperatively
- If intact, these patients may be candidates for phrenic nerve pacing
- Phrenic nerve pacers can be laparoscopically placed, including internal electrodes and an external transmitter
Clinical Scenario:
A 36 year old male sustained a C3 ASIA B SCI 1 week ago He is currently in the ICU being mechanically ventilated with no significant improvement. Prior to his injury, he was living at home with his wife and two young children and working as an investment banker. Physical examination findings include diminished sensation throughout thoracic region and no motor function below level of injury. Patient goals are to return to home and work independently with focus on resuming his role as a father.
PICO Question:
Does diaphragmatic pacing improve respiratory independence and QOL in individuals with spinal cord injury as compared to mechanical ventilation.
Search Strategy:
21 articles identified using PubMed, CINAHL and Cochrane.
Variations of Terms Used: “spinal cord injury”, “diaphragm pacing”, “respiratory”, “phrenic nerve”
Inclusion Criteria: Diagnosis of cervical spinal cord injury, ventilator dependence, English studies, published 2005-present
Exclusion Criteria: Diagnosis of Amyotrophic Lateral Sclerosis, phrenic nerve lesions
Results:
| Author
Year Country |
Patient Population | Study Type and Level Of Evidence | Outcomes | Key Results |
| Tedde ML, et. al. (2012)
Brazil |
Ventilator dependent quadriplegics post cervical trauma | Clinical Trial
Level 3 Evidence D&B: 12/27 |
Independence from MV3 | •N=5
•At 6 month f/u: •3 patients continuous DPS4 •1 patients 6 hours/day •1 patient unable to sustain |
| Romero FJ, et. al. (2012)
Spain |
Ventilator Dependent High-Cervical SCI patients | Retrospective Review
Level 3 Evidence D&B: 17/27 |
SF-36 | •Social Functioning:
•PNP: 7.67 ± 1.80 •MV Group: 5.67 ± 1.17 •P value <.001 •No significant change in physical functioning, general health, role limitations, physical pain, vitality |
| Poluszny JA, et. al. (2013)
United States |
Ventilator dependent SCI patients with intact phrenic nerves | Retrospective Cohort Study
Level 3 Evidence D&B: 16/27 |
Independence from MV3 | •N=22
•18 participants continuous DPS4 •2 participants: 4 and 12 hours/day •1 patient unable to sustain •1 patient with prolonging life measures withdrawn |
| Hirschfeld S, et. al. (2008)
Germany |
SCI patients with induced respiratory device dependency | Prospective Cohort Study
Level 3 Evidence D&B: 20/27 |
Patient and Physician reported QOL | •Unanimous patient reported improved self confidence with PNP over MV |
| Onders RP, et. al. (2007)
United States |
Ventilator dependent tetraplegics with a C2 injury occurring in childhood | Prospective Cohort Review
Level 3 Evidence D&B: 9/27 |
Independence from MV3, Patient reported QOL | •N=10
•4 patients continuous DPS4 •4 patients day time only •2 unable to sustain •Unanimous patient reported preferences for DPS4, improvements in mobility and ease of integration into society |
Limitations:
- Lacking validated outcome measures
- Small Sample Sizes
- Procedures for implantation and weaning were variable
- Lacking long term follow up
- No control groups
- Lack of homogeneity amongst groups
- Age
- Time on MV
- Level of injury
- Severity of Injury
Clinical Bottom Line:
There is low-level evidence that suggests phrenic nerve pacing is a safe and effective alternative treatment for ventilator dependent, high-level, cervical spinal cord injury patients. Additionally, this evidence supports decreased complications common with mechanical ventilation and improved resocialization, mobility, independence, and overall quality of life.
Phrenic nerve pacing has been shown to improve independence and quality of life. Due to my patient’s goals of returning to his work and family responsibilities, and the lack of any serious adverse events reported with this treatment, phrenic nerve pacing may be an appropriate alternative. After transcutaneous nerve testing determines the patency of his phrenic nerve, offering this as a potential alternative treatment to chronic mechanical ventilation allows my patient to be an active participant in his plan of care.
Acknowledgements:
Thank you to Dr. Richard Lauer for your assistance along the way.
References:
- Posluszny JA, Onders R, Kewin AJ, Weinstein MS, Stein DM, Knight J, et al. Multicenter review of diaphragm pacing in spinal cord injury: Successful not only in weaning from ventilators but also in bridging to independent respiration. J Trauma Acute Care Surg. 2014;76(2):303-9. Doi:10.1097/TA.0000000000000112
- Romero FJ, Gabarrutta C, Garcia-Forcada A, et al. Long-term evaluation of phrenic nerve pacing for respiratory failure due to high cervical spinal cord injury. Spinal Cord. 2012; 50(12): 895-8. Doi: 10.1038/sc.2012.74
- Tedde ML, Filho PV, Hajjar LA, Almeida JP, Flora GF, et. al. Diaphragmatic pacing stimulation in spinal cord injury: anesthetic and perioperative management. Clinics. 2012. 67(11). Doi: 10.6061
- Hirschfeld S, Exner G, Luukaala T, Baer GA. Mechanical ventilation or phrenic nerve stimulation for treatment of spinal cord injury-induced respiratory insufficiency. Spinal Cord. 2008; 46(11): 738-42. Doi: 10.1038/sc.2008.43
- Onder RP, Elmo MJ, Ignagni AR. Diaphragm Pacing Stimulation System for Tetraplegia in Individuals Injured During Childhood or Adolescence. J Spinal Cord Med. 2007; 30(1):25-29.
With further questions please contact Rebecca Maidansky at rmaidansky@temple.edu