Background:
Depression affects over 120 million people worldwide. Major depression disorder is one of the most common mental disorders in the United States and it is estimated that by the year 2020 it will be second only to coronary artery disease for disability-adjusted life years lost for both sexes.
Currently, the first option for the treatment of depression is antidepressant medications, which are shown to have significant side effects
Case Scenario:
My patient is a 45 y/o female who presents to physical therapy with a primary complaint of chronic low back pain (LBP). She is a single mother of 3 and currently works as a lawyer. She reports high levels of stress and decreased activity; she used to be an avid runner and tennis player. Patient has a PMH significant of depression. She participated in PT for 4 weeks with only marginally improvements in disability index score. Patient continues to complain of LBP. In addition, pt now complains of fatigue, weight loss and trouble sleeping. Therefore, severity of depression outcome measures implemented.
Clinical Question:
In adults with depressive disorder is moderate intensity aerobic exercise a MORE effective treatment compared to traditional treatment in decreasing depressive symptoms and increasing QOL?
Two outcome measures were analyzed :
- Severity of Depression Scale: Hamilton Depression Rating Scale (HAM-D); Beck Depression Inventory-II (BDI-II)
- Quality of Life: WHO Quality of Life- BREF (WHOQOL-BREF)
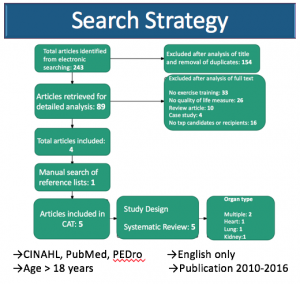
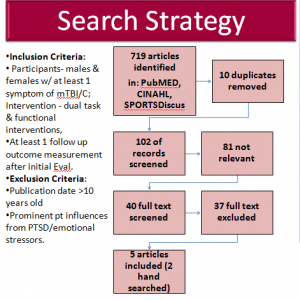
Search Strategy:
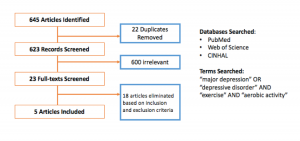 Inclusion Criteria:
Inclusion Criteria:
Articles within 10 years (2006-2016); diagnosed with a depressive disorder; Adults 18 and older; moderate intensity exercise; article had to compare either exercise and usual care to medication OR compare exercise to medication
Exclusion Criteria:
Presence of another primary psychiatric disorder (bipolar disorder, anxiety etc.); medical co-morbidities (diabetes, CHF etc.)
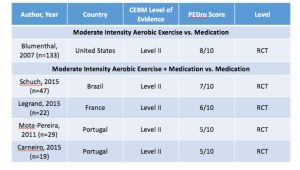
Levels of Evidence:
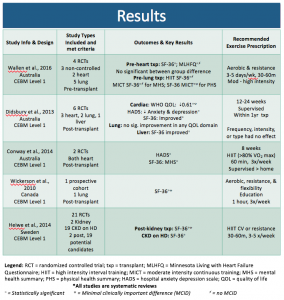
Results- Aerobic Exercise vs. Medication:
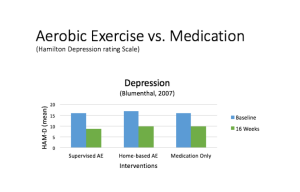 Graph 1:
Graph 1:
The only article that looked at AE vs. Medication was by Blumenthal at al. The graph represents the mean difference in HAM-D scores between the two groups at 16 weeks. There was no statistical difference between groups, however there was statistically significant changes in severity of depression scores within all groups. This shows that Moderate intensity aerobic exercise (AE) could be as effective as medication only.
Results: Aerobic Exercise + Medication vs. Medication
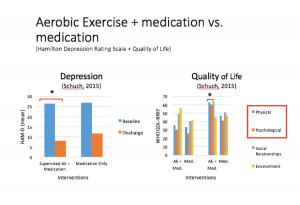 Graph 2:
Graph 2:
This graph on the left represents the mean difference in HAM-D scores between two groups at discharge (Avg. LOS= 3 weeks) The asterisks sign represents statistical significance. There was a larger reduction in depressive symptoms in the AE + medication group compared to the medication only group. In addition, the decrease in depressive symptoms for the exercise group were considered clinically meaningful.
The graph on the right represents the difference in QOL between the groups at discharge. There was a larger increase in the QOL score in the AE + medication group compared to the medication only group for only 2/4 domains (physical and psychological domains).
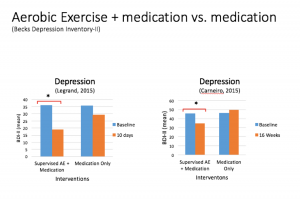 Graph 3:
Graph 3:
These two articles by Legrand and Carneiro, looked specifically at the Becks Depression Inventory. The two graphs represent the mean difference in BDI-II scores between the two groups at 10 days for Legrand and 16 weeks for Carneiro. The asterisk sign represents statistical significance. Meaning there was a larger reduction in depressive symptoms in the AE + medication group compared to the medication only group. In addition, the decrease in depressive symptoms for the exercise group were considered clinically meaningful.
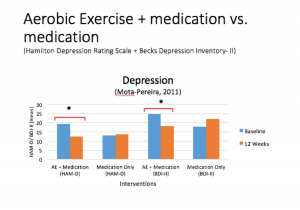 Graph 4:
Graph 4:
This graph represents the mean difference in HAM-D scores and BDI-II scores between the two groups at 12 weeks. There was a larger reduction in depressive symptoms in the AE + medication group compared to the medication only group for both the HAM-D and BDI-II. In addition, the decrease in depressive symptoms for the exercise group were considered clinically meaningful.
Clinical Bottom:
Severity of Depression:
- 1 out of 1 articles shows that AE is equally as effective as medication in reducing depressive symptoms.
- 4 out of 4 articles show AE + Medication is more effective than Medication alone in reducing depressive symptoms. In addition, the 4 out of 4 articles are considered clinically meaningful.
Quality of Life:
- 1 out of 1 articles AE + medication is more effective than medication alone in increasing QOL in 2/4 domains: Physical and Psychological domain.
Limitations:
- Small sample size
- Patient volunteers; more motivated to exercise? Therefore, harder to generalize to the population.
- Women only (Carneiro et al). Therefore, harder to generalize to the population.
- Severity of Depression as a secondary outcome measure (Blumenthal et al)
- In addition, further research is needed on Exercise vs. Medication and long-term effects of exercise on depression.
Clinical Application:
Based off of level 2 quality evidence, moderate intensity aerobic exercise is comparable to antidepressant medication in decreasing depressive symptoms and increasing QOL. Exercise has possible effective therapeutic advantages compared to medication as treatment for depression: inexpensive therapy, health benefits, improves general well-being, minimal side-effects.
Application to Case Scenario:
In addition to LBP management an exercise program can be implemented to decrease depressive symptoms.
For example: 3-4x/week for 6–12 weeks (both in clinic and a home-exercise program) for 30–45 minute duration of moderate intensity aerobic exercise (brisk walking, running, stationary cycling, swimming). In addition, treating co-morbidities such as depression may improve functional outcome measure for the primary complaint (LBP). Furthermore, it is important to encourage the patient to continue exercising after the exercise program is complete to continue to benefit from the benefits of aerobic exercise on depression.
References:
- Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and Pharmacotherapy in the Treatment of Major Depressive Disorder. Psychosomatic Medicine. 2007;69(7):587-596. doi:10.1097/psy.0b013e318148c19a.
- Carneiro LS, Fonseca AM, Vieira-Coelho MA, Mota MP, Vasconcelos-Raposo J. Effects of structured exercise and pharmacotherapy vs. pharmacotherapy for adults with depressive symptoms: A randomized clinical trial. Journal of Psychiatric Research. 2015;71:48-55. doi:10.1016/j.jpsychires.2015.09.007.
- Legrand FD, Neff EM. Efficacy of exercise as an adjunct treatment for clinically depressed inpatients during the initial stages of antidepressant pharmacotherapy: An open randomized controlled trial. Journal of Affective Disorders. 2016;191:139-144. doi:10.1016/j.jad.2015.11.047.
- Mota-Pereira J, Silverio J, Carvalho S, Ribeiro JC, Fonte D, Ramos J. Moderate exercise improves depression parameters in treatment-resistant patients with major depressive disorder. Journal of Psychiatric Research. 2011;45(8):1005-1011. doi:10.1016/j.jpsychires.2011.02.005.
- Schuch F, Vasconcelos-Moreno M, Borowsky C, Zimmermann A, Rocha N, Fleck M. Exercise and severe major depression: Effect on symptom severity and quality of life at discharge in an inpatient cohort. Journal of Psychiatric Research. 2015;61:25-32. doi:10.1016/j.jpsychires.2014.11.005
 References
References