Background
- Extracorporeal Membrane Oxygenation (ECMO) is used as a temporary life support in patients with end stage pulmonary and/or cardiac failure. Due to the limited number of organs available for children, ECMO can be used as a method to extend the life of a suitable candidate allowing them more time on the transplant list.
- Historically, ECMO was the strongest negative predictor of one-year survival post-lung transplant with a major contributing factor being secondary complications associated with prolonged immobility and bed rest. With advances in technology, awake and ambulatory ECMO is now a feasible option.
- Two main types of ECMO:
- Veno-Venous (VV) ECMO Veno-Arterial (VA) ECMO
Case Scenario & PICO
Case: 10-year old female admitted to the hospital secondary to CF exacerbation. Conditioned continued to worsen until she reached respiratory failure and was placed on mechanical ventilation. Despite FiO2 at 100%, patient remained hypercapnic and hypoxic resulting in medical sedation and implementation of VV-ECMO. Patient was placed on the urgent bilateral lung transplant (BLTx) list.
PICO: Do pediatric patients awaiting a lung transplant (LTx) have improved functional outcomes and reduced hospital length of stay if they receive ambulatory ECMO as a bridge to LTx compared to those who receive traditional non-ambulatory ECMO?
Search Strategy
Databases Searched: PubMed, CINAHL, OAIster
Inclusion Criteria: English language, Human subjects, All age groups, Ambulatory ECMO, ECMO as a bridge to heart and/or lung transplant
Exclusion Criteria: Clinical Commentary/Narrative Review, Duplicate in Systematic Review, Non-ambulatory ECMO, Intervention focused on post-transplant ambulatory ECMO, Ambulatory ECMO awaiting a non-lung transplant.
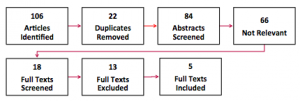
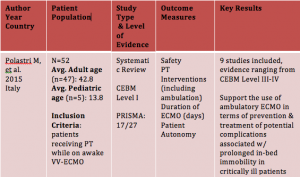
Results

Limitations
- Low quality evidence
- Small sample sizes
- Time and type of PT interventions varied across studies
Clinical Bottom Line
- There is limited, low quality evidence that suggests that ambulatory ECMO improves functional outcomes and reduces hospital LOS in pediatric patients awaiting a lung transplant.
- Ambulatory ECMO is complex and high-risk and should only be performed within a multidisciplinary team in hospitals with ample experience to ensure optimal safety.
Application to Case
- Initiate the conversation with the medical team regarding the benefits associated with immediate PT following ECMO initiation. It will be a multidisciplinary team effort to provide active rehabilitation while on ECMO in order to guarantee safety.
- POC: Initiate PT immediately following initiation of ECMO progressing from PROM while patient is weaning off medical sedation (avoiding ROM of affected limb) –> active exercises in bed –> resistance exercises –> task specific exercises including ambulation until organ transplant.
Acknowledgments
Richard Lauer, PhD and TU DPT class of 2017
References
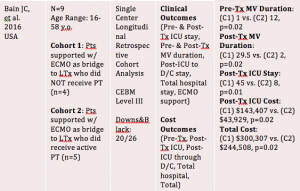
- Bain JC, Turner DA, Rehder KJ, et al. Economic outcomes of extracorporeal membrane oxygenation with and without ambulation as a bridge to lung transplantation. Respir Care. 2016;61(1):1-7. doi: 10.4187/respcare.03729 [doi].
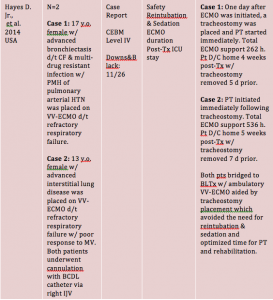
- Hayes D,Jr, Galantowicz M, Preston TJ, Lloyd EA, Tobias JD, McConnell PI. Tracheostomy in adolescent patients bridged to lung transplantation with ambulatory venovenous extracorporeal membrane oxygenation. J Artif Organs. 2014;17(1):103-105. doi: 10.1007/s10047-013-0738-9 [doi].
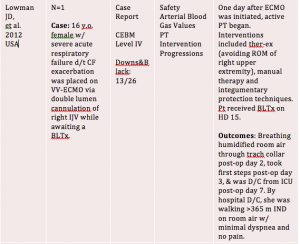
- Lowman JD, Kirk TK, Clark DE. Physical therapy management of a patient on portable extracorporeal membrane oxygenation as a bridge to lung transplantation: A case report. Cardiopulm Phys Ther J. 2012;23(1):30-35.
- Polastri M, Loforte A, Dell’Amore A, Nava S. Physiotherapy for patients on awake extracorporeal membrane oxygenation: A systematic review. Physiother Res Int. 2015. doi: 10.1002/pri.1644 [doi].
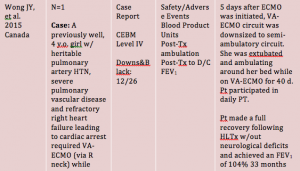
- Wong JY, Buchholz H, Ryerson L, et al. Successful semi-ambulatory veno-arterial extracorporeal membrane oxygenation bridge to heart-lung transplantation in a very small child. Am J Transplant. 2015;15(8):2256-2260. doi: 10.1111/ajt.13239 [doi].
VV-ECMO and VA-ECMO Pictures: http://tele.med.ru/book/cardiac_anesthesia/text/gr/gr031.htm
By: Erika Shumock, SPT